|

Career Fire Fighter Dies After Falling From Tailboard and Being Backed Over by Engine - California
SUMMARY
On August 14, 2004, a 25-year-old female career fire fighter (the victim) died
when she apparently fell from the tailboard and was backed over by an engine.
The victim and her crew had been released from the scene of a residential fire.
The road was blocked by other apparatus, so the victim’s crew began backing
to an intersection approximately 300 feet away in order to proceed forward.
The victim took her position on the tailboard as the “Tailboard Safety
Member” and signaled the driver to begin backing. A Captain acting as
the “Traffic Control Officer” guided the backing operation from
the road on the driver’s side, behind the apparatus, by using hand signals.
When the Captain turned and walked into the intersection to stop cross-traffic,
the victim apparently fell from the tailboard and was run over by the engine.
Members on the scene provided advanced life support and the victim was transported
to a local hospital where she was pronounced dead. NIOSH investigators concluded
that, to minimize the risk of similar occurrences, fire departments should:
- modify existing policies to prohibit members from riding on the tailboard
or any exposed position when the vehicle is in motion
- develop, implement, and periodically review standard operating procedures
for backing fire apparatus
- consider equipping apparatus with safety equipment such as mirrors, automatic
sensing devices, and/or video cameras to assist with backing operations
|
INTRODUCTION
On August 14, 2004, a 25-year-old female career fire fighter (the victim)
died when she apparently fell from the tailboard and was backed over by her
engine. On August 16, 2004, the U.S. Fire Administration (USFA) notified the
National Institute for Occupational Safety and Health (NIOSH) of the fatality.
On January 5 through January 7, 2005, a Safety and Occupational Health Specialist
from the NIOSH Division of Safety Research investigated the incident. Meetings
were conducted with officers of the fire department. Interviews were conducted
with officers and fire fighters who were at the incident scene. The NIOSH investigator
reviewed the department’s standard operating procedures (SOPs), the fire
department’s incident report, the victim’s training records, photographs,
and drawings of the incident site. The incident site was also visited and photographed.
Department
The career department involved in this incident is comprised of 3,250 uniformed
fire fighters. The department serves a population of approximately 6 million
residents in a geographic area of about 250 square miles.
Training
The State requires all career fire fighters to complete training equivalent
to National Fire Protection Association (NFPA) Level I. The fire department
provides all new recruits with a 15-week training course conducted at the city’s
fire academy. The victim had approximately 3 months of experience after graduating
from the academy.
Equipment
Engine 83 (Officer, driver/operator, 2 fire fighters)
Engine 100 (Officer, driver/operator, 2 fire fighters)
Engine 273 (Officer, driver/operator, victim, fire fighter)
Engine 293 (Officer, driver/operator, 2 fire fighters)
Truck 73 (Officer, driver/operator, 3 fire fighters)
Truck 93 (Officer, driver/operator, 3 fire fighters)
Rescue Ambulance 93 (Officer, driver/operator, 3 fire fighters)
B10 (Battalion Chief, firefighter/staff assistant)
Weather
The conditions were clear and sunny, with light winds and temperatures in the
low 90’s. The relative humidity was 49 percent.
INVESTIGATION
On August 14, 2004, a 25-year-old female career fire fighter (the victim) died
when she apparently fell from the tailboard and was backed over by an engine.
At 1254 hours, Central Dispatch received a call of a reported structure fire
and dispatched four engines, two trucks, an ambulance, and a battalion chief.
At 1259 hours, crews arrived on the scene and encountered a one room fire in
a one story, single-family dwelling. Crews were assigned to fire attack, search
and rescue, roof operations, interior truck operations, and searching for extension.
The victim’s crew, among the last to arrive at the scene, placed a smoke
ejector at the front door, donned their self-contained breathing apparatus (SCBA),
and entered the structure. The crew pulled ceiling using pike poles for approximately
two minutes searching for fire extension into the attic. The attack operations
were successful and a knockdown was declared at 1305 hours as the fire was contained
to the room of origin.
|
|
The victim’s crew exited the structure and returned to their apparatus
to remove their turnout coats and SCBA. They remained in their turnout pants
and wore their brush jackets to conduct overhaul. The victim used an axe for
approximately 10 minutes on the roof while clearing a ventilation hole.
The crew returned to their apparatus, removed their gear, and rested for a
few minutes as they drank water. The Incident Commander released the victim’s
crew from the incident at approximately 1330 hours, and because of other apparatus
blocking the road, they were forced to back up to leave the fireground (see
Photo #1).
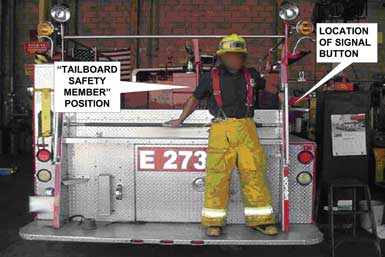
The victim took her position standing on the tailboard as the “Tailboard
Safety Member,” and as directed by department policy, notified the driver
to begin backing up by pushing an electronic signaling button located on the
rear panel of the engine. Note: The fire department policy is for a fire
fighter to ride on the tailboard and guide the driver whenever the apparatus
is backing by pressing a signal button located on the rear engine panel. The
“Tailboard Safety Member” would push the button once to stop, twice
to go, and three times to back-up (see Photo #2 and Photo
#3). The signal button would sound a bell in the cab and a red light would
also flash correspondingly on the dash (see Photo #4).
A Captain, as directed by department policy, acted as the “Traffic Control
Officer” and guided the backing operation from behind the apparatus, in
the road on the driver’s side, by using hand signals.
The driver backed-up the engine at idle speed as they proceeded toward an intersection
where they could turn to go forward. The intersection was approximately 300
feet from where the engine had been parked. The Captain turned and walked into
the intersection to stop cross traffic. At approximately 1343 hours, the Captain
turned back around and did not see the victim. He proceeded across the rear
of the engine to the passenger side while he heard a crashing noise. The driver
saw the Captain cross behind him and looked over to see him in the passenger’s
side mirror. As he was looking in the passenger side mirror, the victim’s
boots came into view on the road through the windshield and he simultaneously
heard the Captain yelling to stop. He immediately stopped and rushed to provide
assistance to the victim approximately 60 feet from the intersection. Advanced
life support was initiated and the victim was transported to a local hospital
at 1355 hours where she was pronounced dead shortly thereafter.
CAUSE OF DEATH
The medical examiner lists the cause of death as multiple blunt force injuries.
RECOMMENDATIONS/DISCUSSIONS
Recommendation #1: Fire departments should modify existing policies to prohibit
members from riding on the tailboard or any exposed position when the vehicle
is in motion.
NFPA 1500 states “All persons riding in fire apparatus shall be seated
and belted securely by seat belts in approved riding positions and at any time
the vehicle is in motion. Standing or riding on tail steps, sidesteps, running
boards, or any other exposed position shall be specifically prohibited.”1
|
|
The department involved in this incident had a policy that required a member
titled the “Tailboard Safety Member,” to ride on the tailboard and
act as a spotter whenever the apparatus was backing. The spotter would face
toward the rear while backing and communicate to the driver with an electronic
signaling button located on the rear panel. A member riding in a standing position
on the outside of the apparatus cannot be secured to provide any means of protection
from a collision or a fall from the apparatus. For an unknown reason, the victim
fell from the apparatus and was run over.
Recommendation #2: Fire departments should develop, implement, and periodically
review standard operating procedures for backing fire apparatus.
Backing a fire apparatus is a challenge regardless of the conditions and should
be avoided whenever possible. If backing is unavoidable, then spotters should
be used to safely direct the operation from outside the vehicle. When backing
the apparatus, all members (excluding the driver and tiller person) should dismount
and act as spotters for the backing operation.2
Spotters should not be permitted to ride the apparatus from an exposed position
such as the tailboard.
The spotters should discuss a backing plan (consistent with the SOP) with the
driver and agree on the communication or warning process prior to beginning.
Communication could be verbal, by a remote electronic signaling device, hand
signals, or radio. The vehicle should not be moved until the spotters are in
position and have communicated their approval to start backing. Once the backing
begins, the spotters should remain visible to the driver. Spotters who are not
in their turnout gear should always wear high visibility reflective vests. At
least one spotter should be positioned at the left rear corner and operate as
the primary spotter. Whenever the driver cannot see the primary spotter, the
backing operation should immediately stop.
Recommendation #3: Fire departments should consider equipping apparatus with
safety equipment such as additional mirrors, automatic sensing devices, and/or
video cameras to assist with backing operations.
Operating a fire apparatus in reverse involves risk of injury as well as equipment
damage.3 Fire apparatus could be equipped or
retrofitted with additional mirrors, commercially available video cameras, or
sensing devices. This would help to alleviate some of the risk involved with
backing operations; however, these devices cannot take the place of spotters,
who are not riding on the apparatus, but assisting and directing the driver
while backing.
REFERENCES
- NFPA [1997]. NFPA 1500, standard on fire department occupational safety
and health programs. Quincy, MA: National Fire Protection Association.
- Phoenix Fire Department [1993]. M.P. 205.08A 05/93-R: standard signals for
backing of fire apparatus. Phoenix, AZ: Phoenix Fire Department.
- U.S. Fire Administration [2003]. Safe operation of fire tankers. Emmitsburg,
MD. Federal Emergency Management Agency FA-248.
|